
March 29, 2020 Update

Dear All,
Apologies for the delay in getting the update out. It was a long week. As many of you know, I myself had COVID 2 weeks ago and fortunately had a mild course, but my Dad also caught COVID roughly 2 weeks ago and had a more difficult course. My symptoms lasted ~3-5 days as outlined here but his course ran close to 14 days with week 2 (this past week) being much worse than the first week. Fortunately he has now turned the corner and recovering well but between monitoring his progress and my usual day job, I got behind on my updates.
The more we learn about COVID, the more we’re seeing folks with prolonged courses and accepting that for some people, their symptoms will last close to 2 weeks before recovery. A New York Times reporter published his own personal bout with COVID with a similar trajectory of close to a 2-week illness requiring hospitalization before turning the corner. This characteristic of the virus is one of many that makes it so challenging to conquer.
Given my absence this week, I have tried to add a lot to this update and hope you find it helpful. I will not be putting another one out until next weekend. I spoke with my home institution, NYU Langone Health, on Friday and as expected they are feeling the surge of COVID patients and need help. Thus, I’ll be heading back to New York this week and taking over as an attending physician on one of the COVID teams starting Thursday.
In my subsequent blogs starting next weekend, I’ll be updating everyone on what I’m seeing on the frontlines from the epicenter of the crisis. Until then, here are my thoughts on where things stand today.
What has changed since last week?
A lot. The US now has the most cases of any country in the world including China. This was to be expected but confirms that the virus will have nationwide impact. No community will remain immune to COVID. Our epicenter is predictably in New York City with others likely to emerge over the next few weeks.
What hasn’t changed is the priority to increase testing capabilities ASAP. We are still behind in our ability to test folks at scale which leaves social distancing / lockdowns as our best solution since we must assume everyone may be infected including those who are asymptomatic.
I do think we’re making progress on the testing front and am hearing a rapid test will be available next week that can detect whether someone has COVID in a matter of minutes. Clearly, it will take time to get this test rolled out at scale, but it’s good to see the progress being made. I’m also hearing the FDA may approve the first serology (blood-based) test to look for antibodies to COVID which would tell you that you’ve been exposed to COVID and now have ‘immunity’ to it. We discussed in our prior blog what we know about immunity but this blood test should be widely available sometime in April and help us identify those who have already been exposed to COVID. The limitation of the serology test is that it takes the body several days before antibodies can be detected in the bloodstream which means the blood test is not helpful in identifying who’s actively infected / contagious in real-time. By the time the blood test is positive, we’ve missed the window for alerting someone they are infectious to others.
Thus, the availability of the blood test won’t change the need for more PCR-based rapid testing with nasal swabs which will tell us who is infected in real-time and enable effective case finding techniques. We need both types of tests and we need both at scale to move forward in controlling this pandemic. This is something to keep a close eye on this week in the news.
The shutdown is starting to really hurt the economy and society at large. Are measures such as lockdowns worth the cost?
This question is likely to be influenced at an individual level based on your unique circumstances such as your risk of severe illness and how much a shutdown impacts your day-to-day life from an economic and lifestyle perspective. Every individual will calculate their own cost-benefit equation based on their unique circumstances. I know we’ve addressed this question before in prior posts, but it understandably remains the question I’m asked the most by folks given the significant impact a shutdown has on local and global economies and day-to-day life.
Here is my answer today with the disclosure that I’m in the healthcare field and have personally gotten the virus along with a family member:
You do not want this virus. Yes, many folks will have a benign, mild course but ~15-20% will not and require hospitalization. One of the scarier parts about this virus is we don’t know who will fall into that 15-20%. We suspect based on data from other countries that the elderly and those with multiple co-morbidities will be the ones that fall into that bucket, but initial data suggests that many of those (~40%) hospitalized are under 55.
Here is a table looking at age ranges in US requiring hospitalization and ICU stays from February 12 – March 16.
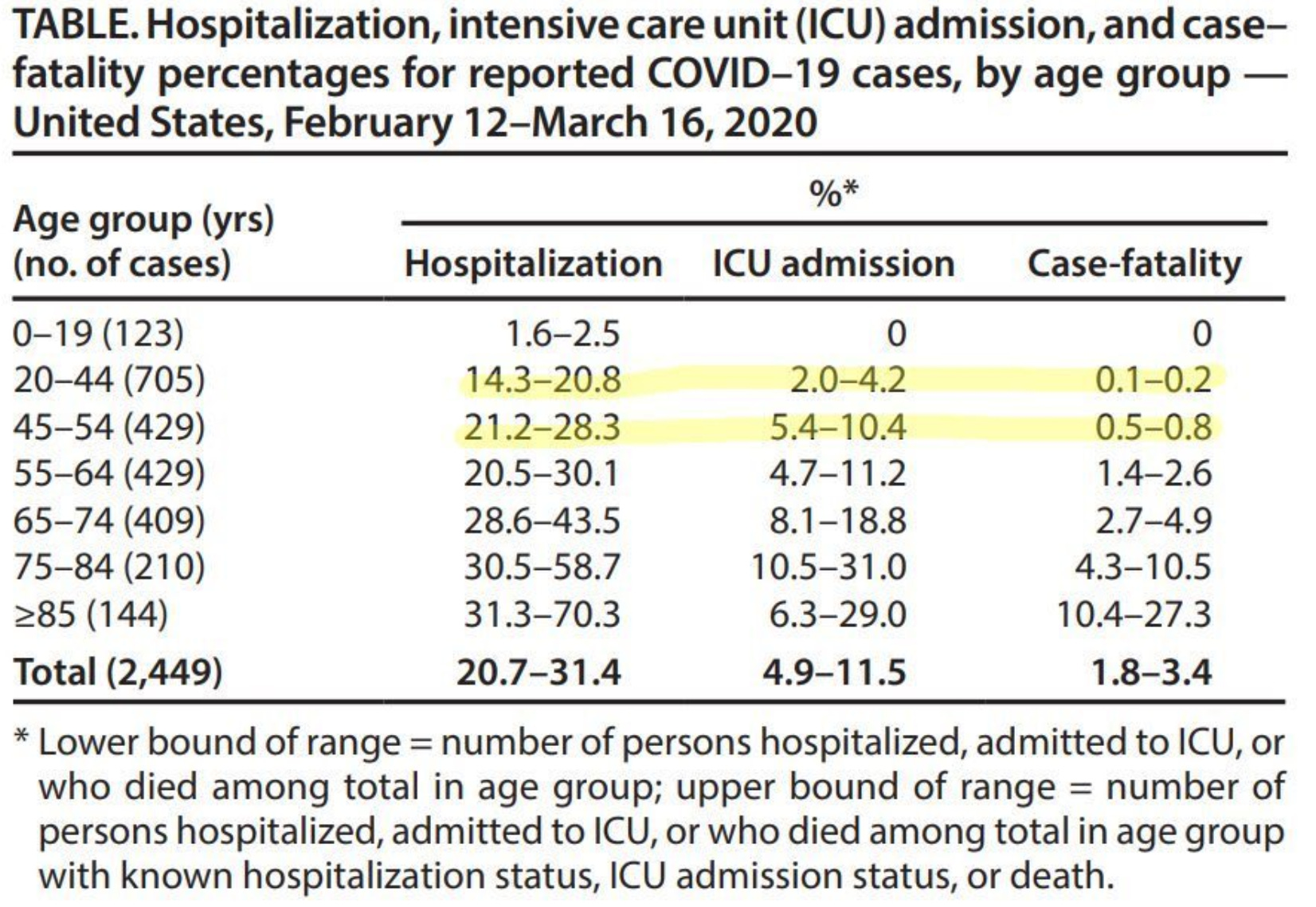

The point is that any of us are at risk of hospitalization or ICU care if we get the virus. When you or a family member are the one who develops a new fever, cough, or tests positive, the best analogy I can give you is you’re setting off on a roller coaster ride that you never wanted to go on. You’re buckled in and you leave the loading bay and you’re off on your own adventure. For some, the journey is uneventful and you get off the ride unharmed with minimal symptoms. You may even find yourself being underwhelmed with COVID because you had minimal symptoms. But, there’s a chance your ride goes off the track and you develop severe enough symptoms and end up in a hospital or the ICU.
Unfortunately, we don’t know why some folks have an uneventful course while others develop severe symptoms. Further, we still don’t have reliable treatments and are mostly left to supportive care and watchful waiting as we work tirelessly to find treatments that work.
We do know that the virus can spread quickly, especially in someone who is symptomatic or someone who is about to become symptomatic. See article here on a ‘super-spreader’ party in Connecticut as the example of a situation where many people were infected from a single, index event and subsequently spread the virus to many other locations. When we go into a shutdown, we dramatically reduce the risk of a super-spreader event and flatten the curve as we discussed in prior posts.
Why do the shut down now especially if my community doesn’t seem to be affected by COVID? Some points to consider:
· Shutting down now buys scientific community time to learn more about this virus so that perhaps if you do catch it in 2 months as opposed to 2 days, we’ll know more about what we can do to prevent your ‘roller coaster ride’ from landing you in a hospital.
· Shutting down now buys us time to produce more personal protective equipment (PPE). As a healthcare system, we’re woefully under-prepared from a supply chain perspective which will hopefully be better in the next few months. If our healthcare workers become infected, we will be unable to treat patients and the mortality rate from COVID will end up being far higher than if we’re able to keep our healthcare workers healthy. Not to mention the obvious personal toll that will take on healthcare workers if they’re exposed to COVID. Having 20 COVID patients in your community hospital versus 200 COVID patients at any given time can’t be understated in terms of the ability to reduce mortality and manage the outbreak. Doing everything possible to keep your community’s hospital census at 20 or less is worth doing.
· Shutting down now buys us time to improve our testing infrastructure discussed above. We will all be much safer going back to ‘business as usual’ once we have the ability to test widely. We don’t have that ability today but hope that we will have that ability in the next few months
Lastly, I haven’t spoken to one healthcare worker who isn’t feeling the strain physically and emotionally from the surge of COVID patients. Stories of having to intubate colleagues such as this tweet below from an ER physician are becoming common place.

Stories of co-workers and colleagues passing away have also begun to surface. I’m sure you can imagine the emotional toll of seeing a colleague pass away from a virus, and then have to go put yourself in harms ways of catching the exact same virus, and then of course, go home and potentially expose your family to that virus. The physical and emotional toll on healthcare workers can’t be over-emphasized.
If we overwhelm our workforce (or our ventilator supply), the mortality rate will be far greater than it would be if the volume of patients was flattened or leveled out over months as opposed to weeks.
Having said all of this, I’m aware that there are significant costs to society to stay shut down. Jobs are lost, folks will have trouble paying bills which will lead to bigger challenges in banking and credit markets, and the harm that will do to the economy. I also know that canceling schools leads to difficult lifestyle changes for everyone having to watch kids 24/7 especially without additional support and perhaps making it difficult to work without child care or being able to have kids in school. This leads to negative societal impact, potentially exacerbating domestic violence, crime, and economic hardship. And, of course, the emotional toll on having to distance from family and friends. These costs are not lost on me and it pains me that this virus has such a high price tag on both the medical and non-medical world. But, it doesn’t change my opinion that the best way to get back to normal is to address the root cause issue of slowing disease transmission.
This virus will impact all of us in some way. We will all be making sacrifices. For some, it will be health sacrifices, for others it will be lifestyle sacrifices, and for many there will be economic sacrifices. No one will come out unscathed. We discussed ‘paying the bill’ in a prior post 2 weeks ago, and, I remain confident that our best hope to return to normalcy as quickly as possible is to hunker down, make our sacrifices now and pay the bill. We only drag out the timeline to getting back to normal if we delay taking action now.
The last thing I will tell you is that each of you will have to define for yourself what is ‘essential.’ I know that everyone is trying to do their part and that everyone is making sacrifices but as we’ve discussed previously, everyone needs to take care of their physical and mental health during this unprecedented time.
Essential things still need to get done and each of you will have to define what is essential and do those things. Essential things for some folks may take the form of needing to visit family or friends to prevent becoming too isolated or lonely. That’s understandable. Again, only you can determine whether seeing family / friends is essential to your physical or mental health. If it is, it’s ok to do that while taking as much precaution as possible. I would still do it in very small groups, keep physical distance as much as possible, wash hands frequently, but you should do the essential things you need to do to stay healthy from a physical and mental standpoint.
Is there any good news?
Yes, there is good news. The social distancing and sacrifices made by many folks over the past 2 weeks is helping. Unfortunately, we can’t let up yet, but there is reason for hope and optimism that we’re making progress. The news above regarding testing is incredibly positive. This doesn’t mean widespread testing will be available tomorrow, but we’re making great strides in testing on both the serology and real-time PCR testing which is an absolute requirement to tame the virus.
Second, we will learn more about how to treat this virus over the coming months. See my below comments on treatment options, but randomized trials are now being conducted in academic medical centers across the country and I’m hopeful we’ll see initial results over the next month.
Third, we still have time to limit spread. Our actions in many states that have gone on lockdown are working to lower transmission. No question the actions from 2 weeks ago to start shutting things down is having a positive impact on slowing the number of infections. The sacrifices we’re all making are having positive impact.
How do we get back to normal?
Scott Gottlieb, who many of you can tell, is my preferred expert on the COVID outbreak recently put out a roadmap for re-opening the country. I agree with his plan and would recommend reading it for those who are interested. A key point is that, each state will be able to re-open at different times based on their unique circumstances of how well the virus is being contained. At the moment, no state is meeting the required milestones to re-open, hence why all states should be strongly considering remaining in lockdown but over the near future, states will start hitting milestones to enter phase 2 of virus containment.
The key milestones that need to be reached are:
· Sustained reduction in number of new hospitalizations for COVID for 14 days in a row. I would focus more on hospitalizations than new cases since no state is testing at scale. Thus, looking at new cases is less reliable than looking at new hospitalizations.
· Local hospital capacity remains adequate. This means that even if cases are going down for 14 days in a row, hospital capacity must be adequate to consider moving to phase 2
· Capacity exists in the state to test everyone with symptoms and state health department has capacity to track/monitor positive cases.
These are the key performance indicators you can monitor in your home state to see how close your state is to moving back towards safely re-opening. Each state will move at different speed towards these milestones but this should give you goalposts to track to see how fast/slow your state is moving towards re-opening.
Clearly, no state is ready for phase 2 today. But, we will get there. Stay strong, keep the faith, and know that we will eventually get back to ‘normal.’ These goalposts are achievable and local/state/federal officials should be working in tandem with the private sector to achieve these milestones, but we need to keep doing our part and making our individual sacrifices in whatever way that looks like until we get closer to achieving these goals.
Any updates on treatments?
Yes. There are multiple randomized trials that are starting at Academic Medical Centers across the country for drugs such as Remdesivir, Tocilizumab, Sarilumab, and hydroxychloroquine to name a few. Treatments are aimed at one of two goals:
Goal #1 is to act as a a direct antiviral agent that fights COVID directly. Remdesivir is an antiviral medication initially designed to treat Ebola and is likely our most promising antiviral agent we are about to start testing in randomized trials. I am hopeful we’ll have preliminary data sometime in April but it’s too early to know for sure.
Another antiviral possibility is to use antibodies from people who have previously gotten COVID and infuse those antibodies into people who are severely ill with COVID to see if those antibodies can help eliminate the virus. The scientific term for this is called using convalescent plasma and it has worked in treating some illnesses previously. Various academic centers in the US are starting to collect blood from those who have gotten the virus and will begin trials studying what happens when we infuse that blood into critically ill patients. A very small study from China was just published in JAMA and looked at 5 patients who received this treatment and showed some promise, but it’s still too early to know.
Goal #2 is to minimize someone’s inflammatory response as the virus can trigger an ‘immunological storm’ where the immune system overreacts and leads to severe symptoms such as fever and respiratory failure. Sadly, it may actually be your immune system’s overreaction causing the damage as opposed to the virus itself. Thus, a potential treatment strategy is to cool down someone’s immune system to limit damage to the lungs and body.
We see this same pathology in other illnesses and have treatments that help tamp down the immune system. We are particularly hopeful that IL-6 blockers such as Tocilizumab and Sarilumab may help modulate a person’s immune response with the hope that they lessen the severity of illness by tamping down a person’s immune response which may be helpful in treating COVID. Again, more time will be needed to study whether this strategy works or not.
We discussed hydroxychloroquine (plaquenil) in a prior post and think it may have antiviral and immune-blocking properties that may be helpful in COVID and trials have started with this drug as well.
The bottom line is that we do have potential treatment options and all of us should remain hopeful that one or many of these agents will prove out to be beneficial in treating COVID. But, we don’t know right now because we don’t have any data to uncover what’s working and what doesn’t. Although all of these treatments may have positive benefits, they all come with side effects and the possibility exists that we do more harm than good by giving any of these experimental treatments.
Thus, the only way to know with confidence whether these treatments do more good than harm is to run randomized trials to test whether these drugs work. You will inevitably hear anecdotes or see a news report of a drug working here and there but remember that without studying these drugs in a structured way, we’ll never know whether it was the drug that made someone better or if the person was going to get better regardless. Further, we need structured studies to learn when is the best time to give a drug and at what dose.
As you can tell, there are many questions to be answered regarding treatment and buying the scientific community time will be enormously important in dictating our ultimate mortality rates from COVID. Slowing disease transmission today remains our best strategy to minimizing the ultimate death toll from this virus.
In closing, I want to re-emphasize how unprecedented these times are in our lives. We have never seen anything like this and will hopefully never be this unprepared for a future pandemic going forward. I know we are all making sacrifices and times are difficult, but stay strong, stay hopeful, and trust that we will get through this and life will return to normal.
Thanks for your comments of support, the articles you send, and well wishes over the past two weeks. We will all need to continue supporting each other in the months ahead.
Stay safe and be well,
Harry
Additional articles of interest for those who want to read more:
Column by Ken Herman on his experience with COVID
Daily Updates from Columbia Chair of Surgery